







")



Affiliate Disclaimer
Some links in this article are affiliate links. We may earn a small commission if you make a purchase through these links, at no extra cost to you. We only recommend products we find useful to our readers
The internet is going berserk asking this question, but most important is to first inform yourself of the science of COVID-19 vaccines! This article explains why the scientific community is not united yet on the use of m-RNA or vector-based COVID-19 vaccines of babies, and how a delayed second dose has come into the picture.
Fatality is the word for it or the silent killer, “happy hypoxia”, very low levels of oxygen in the blood. There is fever, the main symptom of SARS-CoV 2, but hospitalisations are not always necessary. The current 7-day average for May 5–May 11 was 4,049, according to the Centre for Disease Control and Prevention (CDC).
But within 5 days if symptoms do not improve, one must take precaution and get admitted. It is true that the death rates are still quite high. It typically takes a few weeks for the body to build immunity after the first shot (protection against the virus that causes COVID-19). It’s possible that a person could be infected with the virus that causes COVID-19 just before or just after vaccination and still get sick. This is because the vaccine has not had enough time to provide protection. So it may not appear like it is time, but in 10 days or so results are produced.
Vaccine Hesitancy
Around 40 percent of the US is unvaccinated as mentioned above. Reasons are the myths and facts about COVID-19 vaccines. Some people even have bizarre questions like “Can I go for two different vaccines for each dose?” And yes, not every vaccine can work when mixed, but researchers “believe it” can be done with those that share the same target — in this case the “virus’s spike protein”. The mixed regimen is known as a “heterologous boost”. But this is completely going to the individual’s own responsibility.
This question is answered in theory by Prof Sucharit Bhakdi (Thai-German microbiologist) whose field is Bacteriology, Atherosclerosis. He explains the flux in his book Corona, False Alarm? Facts and Figures co-authored by Karina Reiss who has an accolade and PhD in the field of cell biology, biochemistry, inflammation, and infection.
He very well explained how the vaccine contacts our body, the m-RNA vaccine is a gene of the virus which is being introduced into the body which contacts endothelial cells of the blood vessels. This the tapestry layer of the blood stream. The vaccine when recognises the spike (COVID-19 virus) it starts preparing antibodies. But since this is an m-RNA vaccine, it enters into the cell where the spike is. In a normal biochemical reaction, this process clearly produces waste. This waste product is a protein component produced in the opening of the cell. And the immune system lymphocytes get activated.
Creating an immune dependent enhancement of disease, It is when our body has an “overactive immune system”, says Dr Bhakdi. It is not a normal condition, is classified as a disorder. It’s symptoms are fatigue, joint pain and swelling, skin problems and recurring fever. In this light, we cannot keep vaccinating for COVID-19.
We have to understand that if the m-RNA vaccine destroys a virus spike- it is not because it recognises it as Coronavirus. It only recognises it as an unwanted spike and kills it. Which activated T-lymphocytes to kill the cells. These spikes tend to occur where the blood flow is sluggish, like the lungs, throat and nose. But in the future if a person has a real virus-related disease he cannot fight it with the T-lymphocytes that are trained to kill spikes not the cells.
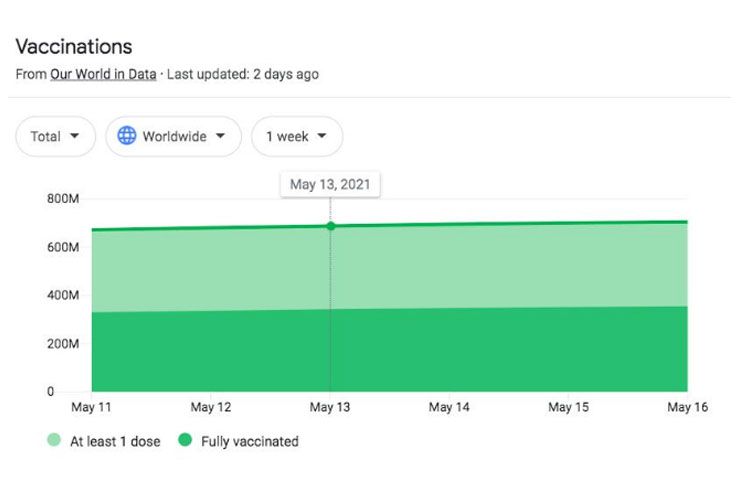
The below image shows how many people have taken a second dose and how many yet to take a second dose.
 Unassailable Contrarieties
Unassailable Contrarieties
Questions were raised in late April this year, after 52 people died after the first dose of AstraZeneca in Europe due to severe cerebral thrombosis. This is why politicians, civil society and researchers are not able to apply mind and scientific research to gather for the benefit of public interest, says Dr Bhakdi.
The urgency for the development of a vaccine is the reason for the paradigm shift in the process development of the vaccine. Many steps of vaccine development have been performed in parallel to save time. As a result, different types of COVID-19 vaccines are emanating from multiple platforms and formulations have progressed rapidly to advanced stages of their final form. Which leads us to the three main points of this thesis of “delayed second shot”.
Every person’s immune response will be different (older people above 65 generally have poor immune system). So no chance of knowing the future consequences. Best is to get the shot if you are being offered one and there is. A slot available.
The “virus’s spike protein” may occur in other parts of the body too which are forbidden like the brain due to the contact with gene-based vaccines, or even the non-gene based ones. Depending on the condition of the patient and his immune system will the response of the patient be to the disease and hence the consequences.
There is no consensus on the fact whether the vaccine will attack on the “virus spike protein” in the blood vessels of the lungs (which is where currently the SARS CoV-2 disease is affecting. Speculation is that maybe in later stages, or the next waves of the pandemic, any external virus entering the body will create the “immune dependent enhancement of disease”, “Which is very bad,” says Dr Bhakdi.
John Sanders, a professor of medicine and chief of the section of infectious disease in the Wake Forest University School of Medicine, said to a Davie County Enterprise reporter, “It was an amazing success in compressing the vaccine process. “It is wrong to think that they invented vaccines 18 months ago and had them approved in less than a year,” he said. “We’ve been doing gene-based vaccine studies since the 90s.”
Experts, Dr William Schaffner, Professor of Preventive Medicine and Health Policy at Vanderbilt University , Dr Sara Fortune, Director of the TB Research Program at the Ragon Institue of MGH, Harvard, and MIT and Children’s Hospital of Philadelphia, released a paper “Antibody-Dependent Enhancement (ADE) And Vaccines” Which has stated that a vaccine would not be approved these days if pathogenic priming was documented. When the COVID vaccines were developed, they were being examined for possible ADE too, WUSA-TV reported Tuesday.
Although, what is “scientific” to say that heterologous boost is the way to go, can’t say. Now, research is taking place to see if so many COVID-19 vaccines could be tested for heterologous prime-boost vaccination strategies in clinical trials to elicit higher and broader protective immune responses (both antibody and T cell responses). The idea is that this will build improved safety profiles. Ordinary non-science people do not make sense of this in a positive way. But yes, this is only to meet emergency needs and may assist in the formulation of public health policies.
What happens to your body when you have taken the first shot and not taken the second shot of the vaccine?
Symptoms of the first dose are splitting headache, nausea, jerky limb movements, dizziness, blood clotting, hard of hearing and blurred vision are some symptoms of the side effects of first dose of the COVID 19 vaccine, especially after Astrazeneca, and Modern. There is no need to fear and panic though, it only means the vaccine is working on your body. But some people who have died, or had a severe case of cerebral thrombosis, might consider not taking the second dose.
The most common treatments are monoclonal antibody therapy or convalescent plasma while ill and who need to wait 90 days before their second dose. Monoclonal antibody (mAb) therapy was introduced when there was no way to combat COVID-19 when it first started to show up everywhere and became a pandemic.
To stop it, monoclonal antibody infusion treatment was given to some individuals who tested positive for the virus were at high risk for developing “severe illness”, said Dr. Howard J. Huang, medical director of the Houston Methodist Lung Transplant Center. The goal of this therapy was to help prevent hospitalisations, reduce viral loads and lessen symptoms’ severity.
Those at risk were those who were 65 years of age or older, at least 55 years of age and have heart disease, hypertension or a chronic respiratory disease such as Chronic obstructive pulmonary disease (COPD), Have a BMI above 35, have chronic kidney disease, diabetic, and are already receiving immunosuppressive treatment or have an immunosuppressi
ve disease.
This new type of therapy relies on “monoclonal” antibodies to attack and kill the virus spikes. These antibodies are similar to the ones your body would naturally make in response to any infection. However, monoclonal antibodies are mass-produced in a laboratory and are designed to recognise a specific component of this (SARS-CORONAVIRUS) virus — the spike protein on its outer shell. By targeting the spike protein, these specific antibodies interfere with the virus’ ability to attach and gain entry into cells. The two monoclonal antibody therapies available in the world right now are the bamlanivimab and a combination of the casirivimab and imdevimab.
In The News
Now, the new policy is “delayed second dose”. Where M-RNA vaccines like Moderna and Pfizer feature, these require two shots for full protection, and most other vaccines too require two doses for full treatment. Dr. Anthony S. Fauci, the director of the National Institute of Allergy and Infectious Diseases has actually said, due to the shortage of vaccines, this is actually a “reasonable approach”. The CDC in its research of health care and emergency workers at high risk for exposure to the coronavirus found a single dose of Pfizer’s or Moderna’s Covid-19 vaccine was 80 percent effective at preventing Covid-19.
But some scientists doubt the methodologies being used. For example, Dr Sucharit Bhakdi, MD from University of Bonn in Germany has pointed this out, through the Pfizer clinical trail case: If there are two human groups of 10,000 each, and 1o people in one group that is vaccinated gets COVID-19 and in the other group of 10,000 which does not get the vaccination have 52 people who get COVID-19, is not a valid test.
However, “The second dose of mRNA vaccines induces a level of virus neutralizing antibodies about 10-fold greater than the first dose,” said Dr. Paul Offit, a professor at the University of Pennsylvania and a member of the Food and Drug Administration’s vaccine advisory panel. “Also, the second dose induces cellular immunity, which predicts not only longer protection, but better protection against variant strains,” the New York Times reported. Fact is it does not matter when you take the second shot. But second shot should not be taken after more than 6 months and it is required for the full treatment of COVID-19- 229E (alpha), NL63 (alpha), OC43 (beta), HKU1 (beta, MERS-CoV, a beta virus that causes Middle East respiratory syndrome (MERS), SARS-CoV, a beta virus that causes severe acute respiratory syndrome (SARS) and SARS-CoV-2.
Each case of COVID-19 is different because there are several virus variants which is infecting people across the world. The current vaccines which are largely being used in clinical trials include Novavax, Sinovac, BioNtech/Pfizer, and Oxford-Astrazeneca across the world, but they are not effective against all variants of the Coronavirus. These vaccines are not yet approved by the Food and Drug Administration for vaccination drive. It has FDA Authorised Pfizer-BioNTech “COVID-19 Vaccine for Emergency Use”. The new double mutant variant B.1.617 is an Alpha Coronavirus Immunity Disease of 2019, 2019 n-CoV, which is part of the Severe Acute Respiratory Syndrome (SARS) family of viruses, which is plaguing the world slowly, in waves, since late 2019. Moreover, this is the second wave of the pandemic, and politicians, doctors, healthcare workers, scientists and media all have their own version of the truth about delayed second dose of the vaccine.
Myths And Facts About COVID-19
1. Q: How do I know which COVID-19 vaccine information are accurate?
A. It can be difficult to know which sources of information you can trust. Before considering vaccine information on the Internet, check from where the information comes from and that it is updated on a regular basis. Ask experts on social media about credible vaccine information sources.
2.Q Should I get a COVID-19 vaccine if I would like to have a baby one day?
A. Yes. No evidence as to why not.
3. Do COVID vaccines alter our DNA?
No. COVID-19 vaccines do not change or interact with your DNA in any way, CDC, reported. There is a myth around gene-based M-RNA vaccines that they are not like the “normal” vector genetic material. But both develop antibodies that will fight the virus.
3. Q. Is COVID-19 vaccine mandatory?
No. The federal government does not mandate (require) vaccination for people. Although, private companies’ rules don’t apply in large constitutional decision-making processes.
4.Q. What if I have viral fever will I test positive for COVID-19?
.None of the authorised and recommended COVID-19 vaccines cause you to test positive on viral tests, CDC has said. Experts are currently looking at how COVID-19 vaccination may affect antibody testing results.
No. None of the authorized and recommended COVID-19 vaccines or COVID-19 vaccines currently in development in the US contain the live virus that causes COVID-19. Sometimes after the first dose there can be symptoms, such as fever. These symptoms are normal and are signs that the body is building protection against the virus that causes COVID-19.
5.Q. Does COVID-19 shreddable components that can affect my menstrual cycle?
No. Menstrual cycles cannot be affected by being near someone who received a COVID-19 vaccine. Those who have received a COVID-19 vaccine shot cannot shed or release any of the vaccine components. None of the vaccines authorised for use in the United States contain a live virus so it is not possible to shed it.
In a Nut-Shell
Doctors are aiming now at lower risk of death. and hence it is vaccine efficacy over long-term health consequences which may arise from new treatments being innovated. For example, New England Journal of Medicine reported, “Among patients hospitalised with Covid-19 who were not receiving mechanical ventilation, transfusion of plasma with higher anti-SARS-CoV-2 IgG antibody levels was associated with a lower risk of death than transfusion of plasma with lower antibody levels”.
On the other hand, COVID-19 convalescent plasma was a goal directed therapy, The medical journal The Lancet on Friday said, an open-label study done in 177 National Health Service hospital organisations in the UK in which 5795 patients received convalescent plasma plus usual care and 5763 received usual care alone in a randomised clinical trial, stated that efficacy of convalescent plasma is not useful for those hospitalised with the virus.
Common structural evaluations through radiological experiments in patients with the SARS-CoV 2 show:
- Ground glass opacities in the affected cells
- Lobes affected by the ground glass opacities
- Consolidation
- Some have nodules
- Reports of pleural effusion
- Abnormal sized lymph nodes
- Lung impairment
Latest research has pointed out that we can afford to take a delayed second does contemplating durability of vaccine-induced protection after the first dose in order to determine the optimal time interval between the 2 doses.
The largest reduction of severe outcomes was achieved with a 9- to 15-week delay in the second dose, according to this study curated by Canadian Institutes of Health Research, TNV: São Paulo Research Foundation; APG, MCF: the National Institutes of Health; and APG: the National Science Foundation.
B.1. 617.2 is now the latest coronavirus variant, and their widespread transmission have led to a public health conundrum regarding whether to vaccinate more individuals with the first dose of available vaccines and delay the second dose or to prioritise completion of the 2-dose series based on tested schedules in clinical trials.
This virus has been found in 44 countries across the world and currently is becoming a cause of panic and fear. Our vaccination doses of Covaxin, Covishield, Oxford-Astrazeneca, Pfizer, Biological E, Moderna, Johnson & Johnson, Zydus Cadila, Novavax, Janssen, Bharat Biotech’s Nasal Vaccine, and Sputnik V are only tested against the beta virus that causes Middle East respiratory syndrome (MERS) first strain, MERS-COV. And amongst others, Novavax-CoV2373 Covid-19 Vaccine is tested against, B.1.351 (South-African variant) COVID mutant variant.
Fact is fact, mass behavioural impacts of social media communications amplifies beliefs held by an individual and also discounting beliefs they do not hold about the coronavirus vaccines. For example, Bristol University research shows, children are showing regressive behaviour after the first COVID-19 shot, and pregnant women with COVID-19 are facing double complications because of hypertension.
It is because science is always evolving, there is no one last answer to COVID-19 vaccines’ story. More tests, new outcomes and further analysis and stepwise advancement.
There have been many surveys to know what percentage chance there that people are happy with COVID vaccine results. A report published in the popular scientific journal The Lancet said, “With approximately 10% of the population who are strongly hesitant about COVID-19 vaccines, provision of information on personal benefit reduces hesitancy to a greater extent than information on collective benefits. Where perception of risk from vaccines is most salient, decision making becomes centred on the personal.”
It seems that most of the public is informed and sceptical about COVID-19 vaccinations.According to Nature magazine website, “The trends are encouraging”. But 44% are still unwilling to receive COVID immunizations in the United States. Deborah Jones, a physician at Columbia University Irving Medical Center in New York City said, “It’s great to see that more people are now open to getting a vaccine.
But what strikes me is how many people are still hesitating. Vaccine hesitancy will slow down our return to normal.” In Japan, around 66% of the people are not trusting the vaccine, because of side -effects and apparent mortality occurring even after the second dose is given. As of now, according to WHO AstraZeneca/Oxford vaccine, Johnson and Johnson, Moderna and Pfizer/BionTech and Sinopharm COVID-19 vaccine for emergency use.
Conclusion
COVID-19 vaccine cannot make you sick with COVID-19, CDC has made clear. There is a possibility that you were pre-symptomatic. In many countries, there is a shortage of vaccines including India. The highest is Mexico with death as on 17th May, 2021 at 9.25. The lowest is Singapore and Bhutan at 0.05 and 0.08 respectively.
These are calculated based on death per million and total deaths in the last 7 days. On the other hand, Poland and Israel have already removed their masks and started their hugging ceremony in their community. The risk of infection for people susceptible to COVID-19 depended on contact with infectious individuals that could be in asymptomatic, pre-symptomatic, or symptomatic stages of the disease.
The health ministries across the globe are aiming at administering approximately 100 million vaccine doses in the first 100 days- this is outlined by the Biden administration, different countries are adopting different measures to control the spread.

